

Gastric ulcers in horses; ECEIM consensus statement
In 2015 the “European College of Equine Internal Medicine (ECEIM)” published the new “consensus statement” regarding gastric ulcers in adult horses.
This “consensus statement” is written by B.W. Sykes, M. Hewetson, R.J. Hepburn, N. Luthersson and Y. Tamzali. It was published in the “Journal of Veterinary Internal Medicine” (29: 1288-1299) and available as “open access” article. Below you can find a summary.
Terminology
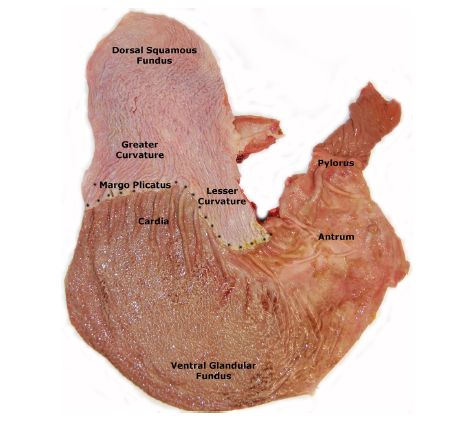
“Equine Gastric Ulcer Syndrome” (EGUS) is the general term used for all erosive and ulcerative diseases of the horse stomach. Based upon the affected regions in the stomach, two categories can be distinguished: “Equine Squamous Gastric Disease” (ESGD) and “Equine Glandular Gastric Disease” (EGGD).
ESGD is further divided into primary ESGD and secondary ESGD. Primary ESGD affects horses with normal gastric emptying, while secondary ESGD occurs in horses with delayed gastric emptying due to underlying pathology such as pyloric stenosis. EGGD is specified further based upon the anatomical location and the appearance of the lesion.
Prevalence
The prevalence of gastric ulcers varies with breed, use and level of training. There is also a difference in prevalence between ESGD and EGGD. ESGD has the highest prevalence in thoroughbred racehorses. The prevalence of EGGD is less well understood. Most lesions of EGGD are found in the antrum pyloricum.
Epidemiology
Several studies show that there is a correlation between the presence of ulcers and the breed. The influence of age and gender is inconsistent which suggests that other factors, such as intensity and duration of training, are more important. Other factors, of which it has been described that they are a possible risk factor, are described below.
- Grazing is shown to decrease the risk of gastric ulcers, but supporting evidence is contradictory.
- Unlimited/frequent access to roughage is considered to reduce the risk on EGUS, but supporting evidence is not available. Besides, findings suggest that the impact of roughage without reduction of other risk factors might be less than expected. The occurrence of ESGD is more likely when straw is the only form of roughage provided. This suggests that also the type of roughage influences the prevalence of ESGD.
- An increased interval (> 6 hours) between roughage meals increases the risk on ESGD, when compared to more frequent (< 6 hours) roughage supply.
- An increased starch intake is consistently associated with an increased risk on ESGD in animals trained at different levels.
- Intermittent water access increases the risk on EGUS.
- Fasting is an often described risk factor for ESGD; intermittent fasting causes ESGD and increases its severity.
More large-scale research is needed to understand the epidemiology behind EGUS, especially behind EGGD.
Clinical symptoms
Stomach ulcers in adult horses are associated with a broad range of clinical symptoms: a decrease in appetite, slower eating, poor body condition score or weight loss, chronic diarrhoea, a bad coat condition, teeth grinding, behavioural changes, acute or recurring colic and bad performance. There is however no strong epidemiological evidence for the correlation between the presence of these clinical symptoms and the occurrence of gastric ulcers.
A broad range of clinical symptoms can occur in individual EGUS cases. On population level the different gradations of a decreased appetite and a poor body condition score are most common. Behavioural changes, including stereotypes, are inconsequent, but not unusual. EGUS can also contribute to bad performance, but considering the number of factors that can contribute to this, other factors should also be taken into account. Differences in clinical symptoms occurring with ESGD or EGGD are currently not known. Despite the large variety of possible symptoms, all these symptoms are badly correlated to the presence of EGUS. Diagnosing EGUS based on the presence of “typical clinical symptoms” should thus be avoided.
Diagnosis
Gastroscopy remains the only reliable ante-mortem method to determine accurately if a horse has gastric ulcers. The entire stomach, including pylorus and proximal duodenum, should be included because lesions in one of these regions are easily missed.
There is no correlation between the presence of ESGD and EGGD. The presence of one cannot serve as an indication for the presence or absence of the other.
There are currently no reliable haematological or biochemical markers that can be helpful in diagnosing gastric ulcers.
Ulcer grading
The 0 – 4 “Equine Gastric Ulcer Council” system is recommended as a standard scoring system for ESGD.
Due to a lack of data to support the validity of the hierarchical grading system for EGGD, the use of this type of grading system is not recommended. For EGGD it is recommended to describe the lesion based on the presence or absence, anatomical location, distribution and appearance.
The biggest challenge is to determine the clinical relevance of the individual lesions found. There is little evidence that the presence and grading of the lesions correlates with the presence of clinical symptoms. The clinician should try to interpret the results of the endoscopy in relation to the complete clinical picture, history, etc.
Pathophysiology
ESGD is caused by an increased exposure of the squamous mucosa to acids. The relation between exposure of the squamous mucosa to gastric content and fasting and training has been described clearly. During gaits faster than a walk, the acid gastric content will be pushed up to the squamous mucosa by the increased intra-abdominal pressure.
The pathophysiology of EGGD, on the contrary, is poorly understood. The glandular mucosa differs fundamentally from the squamous mucosa by the fact that it is exposed to gastric acid in physiological conditions. For this reason it is thought that EGGD is caused by failure of the normal defence mechanisms that usually protects the mucosa against the acid gastric content. There is still no evidence that bacteria are the direct cause of EGGD.
NSAIDs have the potential to induce EGGD in individual animals, but on population level they do not contribute significantly to the prevalence of EGGD. The ulcerogenic capacity of some NSAIDs has been shown when dosages were administered that are 50% higher than the recommended dosages. When the recommended dosages are administered, phenylbutazone and suxibuzone however do not induce gastric ulcers.
It is most likely that a combination of different factors contributes to the development of EGGD in horses.
Treatment and prevention
The therapy of both ESGD and EGGD focuses on adequate suppression of acid production. The proton pomp inhibitor omeprazole is the first choice treatment. Omeprazole is superior to ranitidine.
The duration of acid suppression needed to heal ESGD and EGGD has not yet been described. Clinical studies suggest that a period of 12 hours during which the acid production is suppressed may be sufficient for the treatment of ESGD. GastroGard gives a consistent healing rate of 70-77% when administered at the registered dose of 4 mg/kg per os, once daily, during 28 days. A lower dosage and/or shorter period of administration can however be taken into consideration based on the evidence available.
The success rate of EGGD treatment is only 25%. The reason for this poor response is unknown. A longer duration of treatment may be indicated in the case of EGGD. Bacteria might also play a part. In the absence of evidence to support this theory and in the context of responsible antibiotic use, it is however not recommended to use antimicrobials in the routine treatment of EGGD.
Considering the role of mucosal defence mechanisms failing in the pathogenesis of EGGD, protecting the mucosa as part of the therapy seems legit. Sucralfate is best studied for this indication. The combination of omeprazole (4 mg/kg PO once daily) and sucralfate (12 mg/kg PO twice daily) improves the success rate of EGGD when compared to omeprazole only.
The pharmacological approach of the prevention of ESGD is comparable to the treatment. Omeprazole is used as prevention in a dosage of 1 mg/kg per os, once daily. The efficacy of omeprazole as prophylaxis for EGGD is unclear, but so far there is no difference in the prevention strategy of both.
Nutraceuticals are attractive because of the ease of use and their availability. Pectine-lecithine complexes have been shown to increase the total mucus concentration in gastric juice. Antacids seem to provide some symptomatic relief, but their effect is short-lived.
There is no strong evidence to support a specific nutritional advice. There is only little evidence for the role of the diet in the occurrence of EGGD and therefore the recommendations are primarily based on the well-known risk factors of ESGD. Continuous access to a good quality grass pasture is considered ideal. Unlimited or frequent (4-6 times daily) access to hay (at least 1.5 kg (DM)/100 kg bodyweight/day) can be an appropriate alternative. Straw should not be the only type of roughage, but it can be included safely in the diet with a maximum of 0.25 kg (DM)/100 kg bodyweight. Concentrates should be used as cautiously as possible. Sweet feed should be avoided. The diet should not contain more than 2 gram starch per kg bodyweight per day, or no more than 1 gram starch per kg bodyweight per meal. The interval between feeding concentrates should be at least 6 hours. Maize oil could help to decrease the risk of EGGD development. Water should always be available. When pastes with electrolytes are given orally, they should be diluted in water first, or mixed with the feed.

